Thyroid Nodules
Thyroid nodules are round-oval lumps that develop within the normal thyroid tissue. They are very common; almost half of individuals over 50 years of age will have at least one nodule on ultrasound. Thyroid nodules are 4 times more common in women than in men.
What are the types of nodules?
Thyroid nodules are classified as hot, warm and cold according to the level of thyroid hormones they produce. Hot nodules produce more hormones than the normal thyroid tissue. They cause a clinical condition called hyperthyroidism. Warm nodules produce the same amount of hormones as the normal thyroid tissue and cold nodules produce less hormones than the normal thyroid tissue. Warm and cold nodules do not change the blood hormone levels. Hot, warm and cold nodules can be differentiated only with scintigraphy, which shows the hormonal activity of the thyroid gland and its nodules.
Thyroid nodules can also be classified as cystic, solid or semisolid, according to the ultrasound findings, and also as benign or malignant, according to the biopsy findings.
How are they diagnosed?
Thyroid nodules are generally diagnosed with ultrasound, which is the best imaging modality in thyroid diseases. If a nodule or nodules are seen on ultrasound there are several questions that must be answered:
1. Is the nodule cancerous (malignant) or benign?
2. Is it producing too much thyroid hormone?
3. Is the nodule big enough to cause complaints?
4. Is the nodule growing (likely to cause problems in near future?)
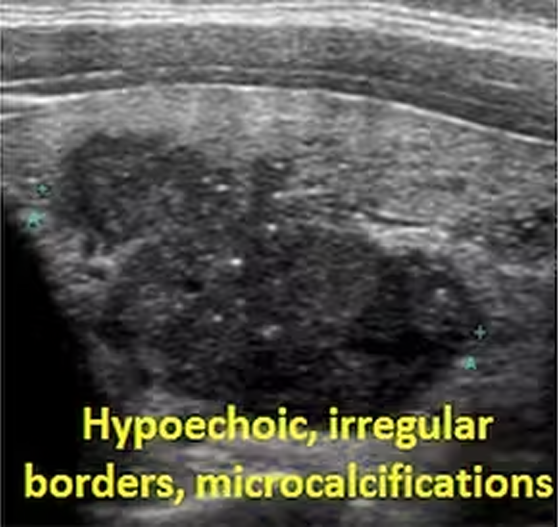
More than 90% of thyroid nodules are benign (not cancer) whereas only 5-10% may prove to be malignant (cancer). Ultrasound can not only show the nodules but also may provide very important information regarding the probability of the nodule being cancerous. Depending on this probability, the doctor will decide whether to perform a needle biopsy or just to follow up the patient with ultrasound. If the following ultrasound signs are present, the probability of cancer will increase:
Solid (not filled with fluid) nodule
Nodule with ill-defined/irregular edges
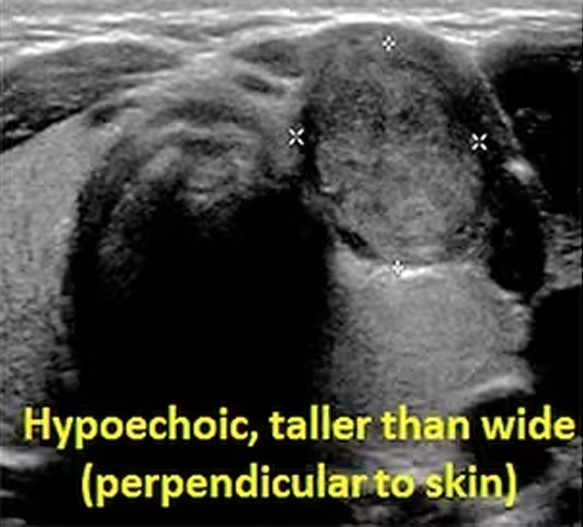
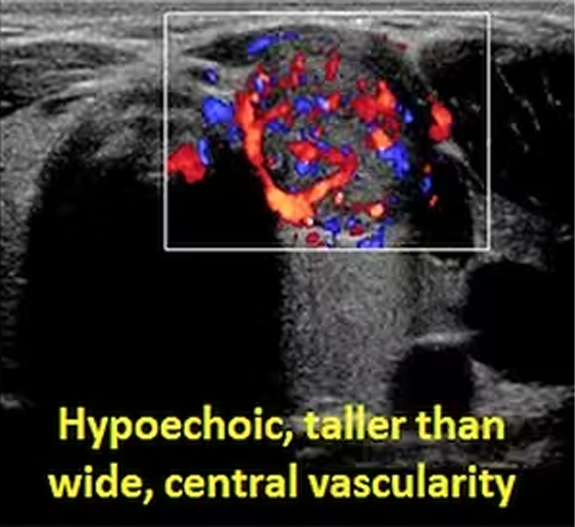
Hypoechoic nodule (looking darker than thyroid)
Long axis of the nodule perpendicular to the skin (taller than wide)
Presence of small calcifications in the nodule
Presence of vessels (vascularity) in the nodule
{kind=link}
{kind=link}
{kind=link}
Some of the common ultrasound features of thyroid nodules that suggest malignancy (cancer).
Why is trucut biopsy better than FNA in some cases?
If the nodule or nodules look suspicious based on above-mentioned ultrasound criteria, then a fine needle aspiration biopsy (FNAB) must be performed. In this non surgical method, a tiny needle is placed into the nodule several times and cells are aspirated into the syringe. The cells are then placed on a microscope slide, stained and examined by the pathologist. Based on the appearance of the cells on microscope, the pathologist decides whether the nodule is benign, suspicious or malignant. In about 15% of FNABs, the amount of cells aspirated is not sufficient to make a diagnosis. In this case, the result is described as “nondiagnostic”.
If the result of the FNAB is nondiagnostic or suspicious, then the biopsy is generally repeated. If the repeat biopsy is done as FNAB + trucut biopsy, the probability of making an accurate diagnosis will be higher. Trucut biopsy obtains cylinders of tissue samples and it is the standart biopsy method in other organs such as breast, liver, kidney and lung. Use of trucut biopsy is challenging in thyroid and thus, not very common. However, in experienced centers, it facilitates the pathologic diagnosis and significantly lowers rate of the unnecessary surgery.
How are benign nodules managed?
If the nodule proves to be benign on biopsy, it may be treated or just followed up. If the nodule is not large, not growing and not causing any problems, then no treatment is necessary and the patient may be followed up with annual ultrasound and clinical examinations. If the benign nodule creates compressive symptoms such as voice changes, shortness of breath and swallowing difficulty, or is larger than 3 cm, or growing continuously on follow up ultrasound exams, then treatment is generally necessary. If the nodule is hot (active), producing too much thyroid hormones and causing symptoms such as sweating, tremor, palpitation and nervousness, then the treatment is necessary regardless of the size of the nodule.
The classic treatment of thyroid nodules is surgery, which involves the partial or total removal of the thyroid gland. However, because of the risk of voice loss (laryngeal nerve damage) and hypoparathyroidism, occurrence of a large surgical scar in the neck and the necessity of life time using of hormone pills, thyroid surgery is not an attractive treatment for most patients. Additionally, removal of the thyroid, which is a functionally important organ, for a benign problem like a thyroid nodule is not acceptible from the scientific point of view.
Because of the disadvantages of surgery, minimally invasive therapies like percutaneous ablation have been introduced and used extensively in the last decades. In percutaneous ablation, a special needle is placed into the thyroid nodule, and the nodule is destroyed either by injecting alcohol (ethanol), by heating (laser, radiofrequency, microwave) or by freezing (cryoablation. Once destroyed, the nodule is shrinked naturally by our body. Six months after the ablation, 60-95% volume reduction is generally observed on ultrasound.
Alcohol ablation is considered the first line treatment in cystic nodules, although it can also be used in solid nodules in selected cases. Thermal ablations such as laser, radiofrequency and microwave or cryoablation destroy the nodule by heating or freezing. They are preferred in solid or mixed (solid + cystic) nodules. All thermal ablations are effective in thyroid nodules, although each has distinct advantages and disadvantages. In our center, we have been using alcohol, laser, RFA and microwave for about 2 decades, and cryoablation and embolization for nearly one decade.
In all cases, we first evaluate the clinical, radiological and laboratory reports of the patient and then decide whether:
- Any treatment is required or not,
- The patient is suitable for nonsurgical treatments or surgery,
- The nonsurgical treatment should be ablation or embolization,
- We should prefer alcohol, heat-based ablations (laser, RF, microwave) or cold-based ablation (cryoablation).
Whatever the method is preferred, ablation has following distinct advantages over surgery:
- It can be done under local anesthesia and ultrasound guidance.
- A thin needle is used for the treatment. There is no incision or suture.
- The risk of the intervention is much lower than surgery
- The risk of voice loss (recurrent nerve damage) is lower because it is possible to control the voice of the patient during the procedure (since the patient is awake).
- The patient can go home 1 hour after the procedure.
- Most importantly, the thyroid gland and its functions are preserved. There is no need for life time thyroid pills.
{kind=link}
{kind=link}
{kind=link}
In our patient with a large solid nodule of the right thyroid lobe, laser ablation was performed. The nodule showed 70% shrinkage at 6 months after the procedure.
Because of these advantages, percutaneous ablation should be the first line treatment in thyroid nodules. Surgery is reserved only if the nodule(s) are not suitable for or have not benefited from percutaneous ablation.
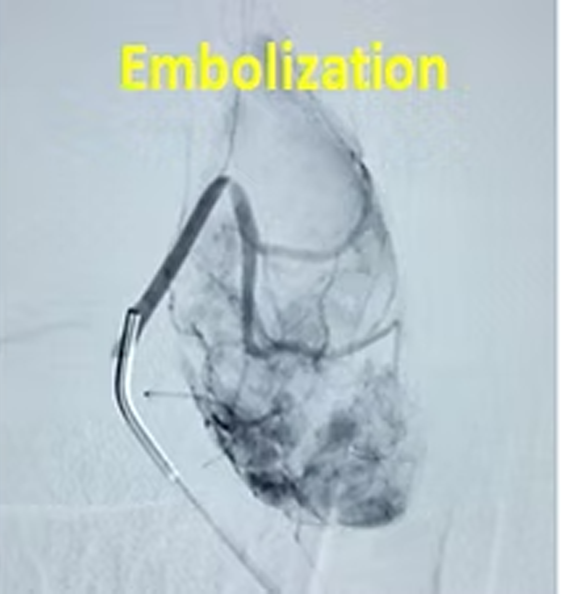
Does embolization have a role in thyroid nodules?
Percutaneous ablation is the preferred nonsurgical treatment in most thyroid nodules. However, sometimes the nodule(s) may be too large (>6cm) or too many (>4-5). In such situations, percutaneous ablation may be less effective or impractical while embolization may become an attractive alternative. In embolization, the feeding vessels of the nodule(s) are occluded with a simple angiography procedure. After the treatment, the nodule(s) shrink significantly and the complaints as well as cosmesis improves markedly.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
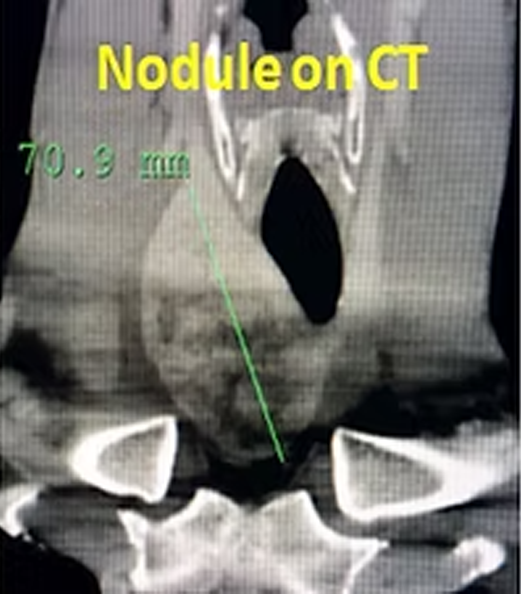
In our patient with a 7cm thyroid nodule, embolization is done instead of ablation because of its large size. Six months later, the nodule shrank by 80% and cosmesis improved markedly.
What should be done if the result of FNAB is nondiagnostic, inconclusive or suspicious?
Sometimes, the result of FNAB may be nondiagnostic, inconclusive or suspicious for cancer. A nondiagnostic result means that there are not enough cells in the biopsy material to make a diagnosis. In this case, the FNAB is generally repeated several weeks later. However, since the insufficient biopsy is generally due to the presence of cyst, blood or hard material inside the nodule, it is quite common that even the second FNAB yields a nondiagnostic result. For this reason, many centers including ours, prefer to perform FNAB + trucut (core) biopsy for the second procedure. Unlike FNAB which tries to suck individual cells into a syringe, trucut biopsy cuts multiple pieces of the nodule, which represent real tissue samples. With combined use of both FNAB and trucut biopsy, the pathologist can make the diagnosis much more accurately and confidently. If the result is cancer, the trucut biopsy materials may also allow identification of the subtype of the cancer with immunochemistry studies.
If the result of the first FNAB is inconclusive or suspicious for malignancy, it is a common practice to operate the patient and remove the thyroid partially or completely. However, the pathology specimens of the thyroid glands reveal no cancer in almost 80% of such patients, which means that the operation was in fact not necessary. For this reason, a second biopsy (FNAB + trucut) is increasingly used in these patients to prevent unnecessary surgery. Recent studies indicate that a FNAB + trucut biopsy can provide an accurate and concrete diagnosis in about 80-90% of these cases, obviating the need of surgery in nearly 50%, which is also the case in our experience. Therefore, we strongly recommend that if the result of the first FNAB is inconclusive or suspicious, a combined FNAB + trucut biopsy be performed, and surgery be reserved for only those cases in whom the combined biopsy is still indeterminate or reveals cancer.
{kind=link}
{kind=link}
{kind=link}
Contact Us
You can get information on our treatments via phone and e-mail as well as by filling and sending the consultation form below. Please send the reports of your thyroid ultrasound, hormones, scintigraphy and biopsy (if available) via e mail (thyroidgoiter@gmail.com) or whats up ( +90-850-255 24 23). Remember to write clearly your e mail address and phone number so that we can return to you as soon as possible.
Please add the reports of your thyroid ultrasound, hormones, scintigraphy and biopsy (if available)