Embolization
Embolization is the intentional occlusion of the feeding vessels of a tumor or tissue for therapeutic purposes. After the procedure, the embolized tissue or organ becomes smaller and the problems it causes may disappear. If the embolized tissue is a tumor, it shrinks or sometimes becomes dead. The complaints it causes either diminish or disappear completely.
Embolization has been using in medicine for more than 50 years for many diseases. Today it is already a popular technique in the treatment of intracranial aneurysms, arteriovenous malformations, uterine fibroids, benign prostatic hypertrophy and liver cancers. Embolization of the thyroid arteries was first reported by Dr Xiao et al in 2002 in 22 patients with Basedow Graves disease. The procedure was successful, and most of the patients had normal thyroid hormone levels after the treatment. Later, embolization was also successfully used in the treatment of large and plunging (going down into the chest cavity) goiters. In our center, embolization is one of the most important treatment options in thyroid diseases, and is used extensively in Graves disease, large goiters, toxic nodular goiters, plunging goiters and large (>6cm) thyroid nodules that are not suitable for percutaneous ablation.
Why we treat large nodules and goiter with embolization?
{kind=link}
{kind=link}
{kind=link}
Large goiters and plunging (going down into the chest) goiters are generally difficult to treat with surgery and also with percutaneous ablation. Embolization is a very attractive treatment option in such patients. In embolization, we occlude the feeding arteries of the goiter and make our body shrink it by time. In many patients, goiters may show 60-80% volume reduction at 6 months, which also continues thereafter. As a result, cosmesis improves and the compressive symptoms caused by the goiter such as hoarseness, shortness of breath and swallowing difficulty may disappear or improve significantly.
Embolization can also be effective for the liver metastases of thyroid cancer. Although RAI is generally the first choice in such situations, embolization or chemoembolization can be effective as a complementary treatment or in patients who respond poorly to RAI.
How to do thyroid embolisation?
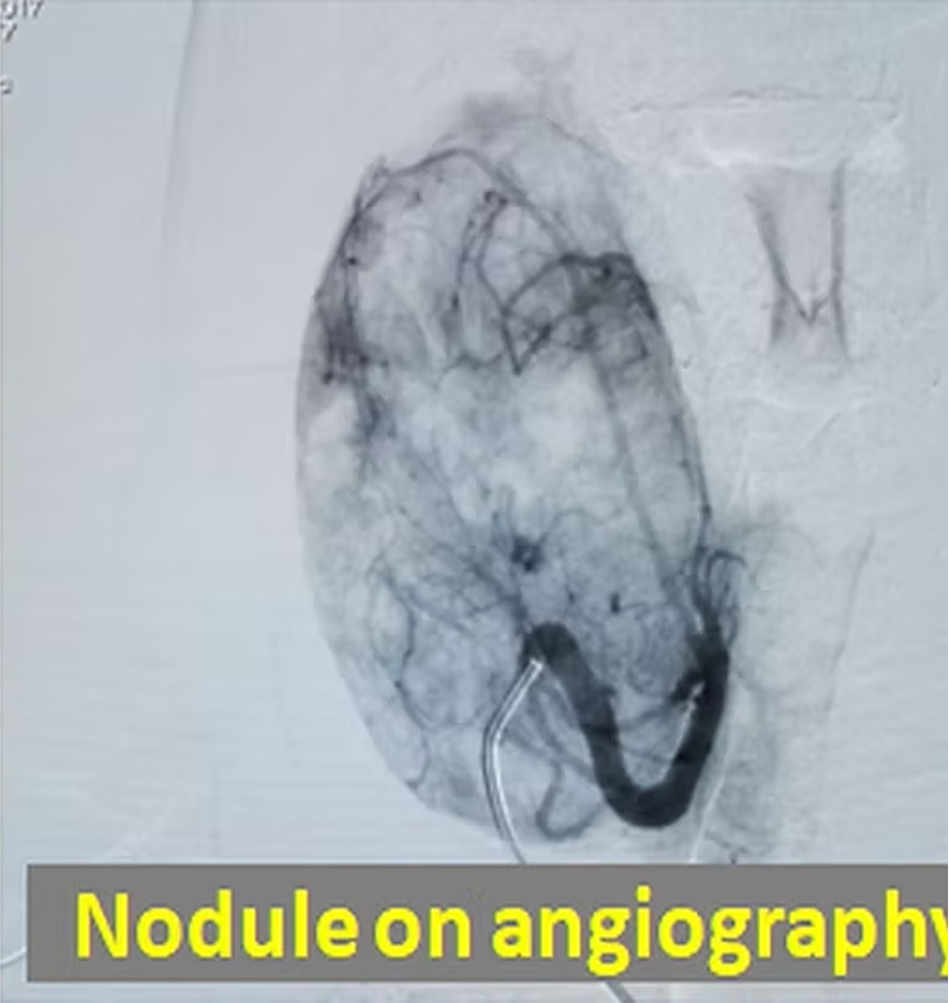
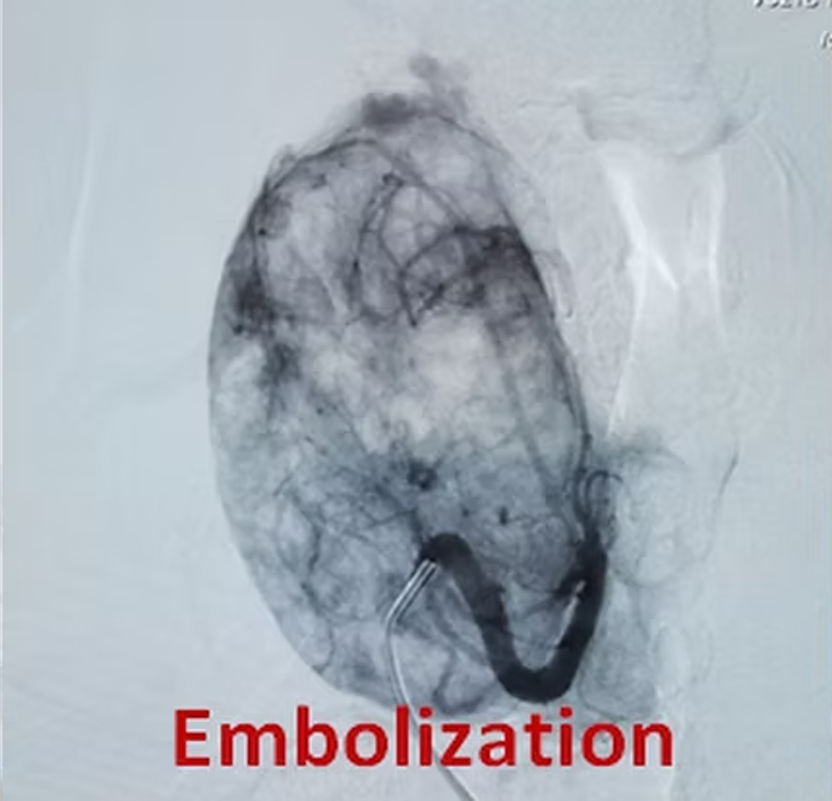
Embolisation is an angiography procedure done with special equipment. The patient is laid on the on the angiography table and the groin is disinfected and numbed with local anesthetic. After a sheath is placed into the femoral artery at the groin, a small pipe called catheter is advanced into the thyroid arteries. After the catheter is placed into the feeding arteries small particle (about half the milimetre in size) are slowly injected and the arteries are occluded.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In our 41 year-old patient with a giant goiter, the feeding vessels of the mass were occluded with angiography (embolization). Three and 6 months after the embolization, two sessions of percutaneous ablation were also performed. The goiter mass has shrank continuously over months, and at one year, the patient had almost a normal-looking thyroid gland on ultrasound.
The thyroid gland has generally four feeding arteries and they also supply four parathyroid glands. This, to prevent hypothyroidism and hypoparathyroidism, 2 or 3 out of 4 feeling vessels are embolized and at least one vessel is left intact. If both thyroid lobes require treatment, embolization can be done first to one lobe, and some months later, to the other lobe. After the embolisation, the thyroid nodules become dead and shrink rapidly. If there is hyperthyroidism as in Graves disease or toxic nodule(s), the TSH, T3 and T4 labels either improve or return to normal. After the embolisation, patients may experience some neck pain and temporary hyperthyroidism for some weeks.
{kind=link}
{kind=link}
Which patients are suitable for embolisation?
In thyroid diseases, the most common treatments are surgery RAI and percutaneous ablation. Embolisation is performed in patients who are not suitable for or do not desire these treatments. For example, in large plunging goiters, surgery is generally difficult since anesthesia is challenging and chest must also be opened besides the neck. In such cases, embolisation may be done easily and effectively. After the procedure, the goiter may become smaller and compressive symptoms such as shortness of breath, swallowing difficulty hoarseness may improve. In Graves disease similarly, embolisation results in lowering or normalization of thyroid hormones in more than 70% of the cases. If the hyperthyroidism is caused by nodule(s) in a MNG patient, embolization can not only make the nodule(s) smaller also correct the hyperthyroidism. Similarly, in patients with a single large (more than 6 cm) nodule, embolisation of the nadule is very effective in reducing its size. In such large nodules, percutaneous ablation is generally not very effective.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
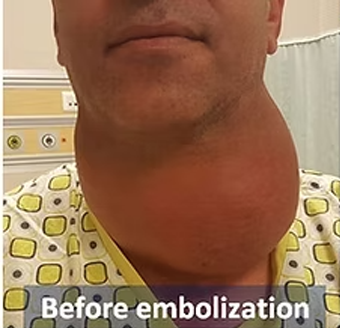
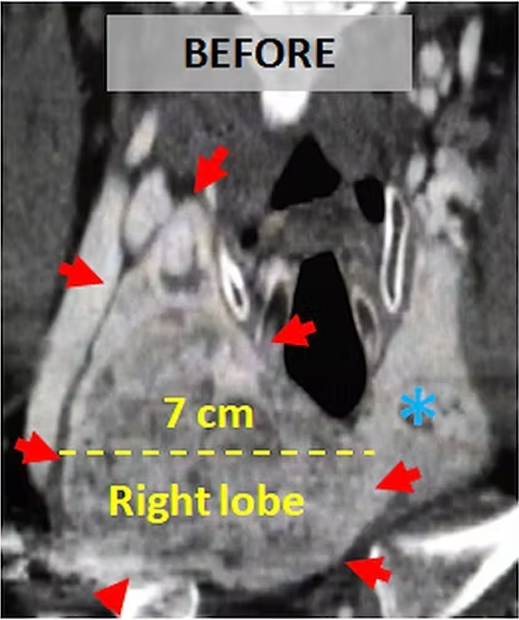
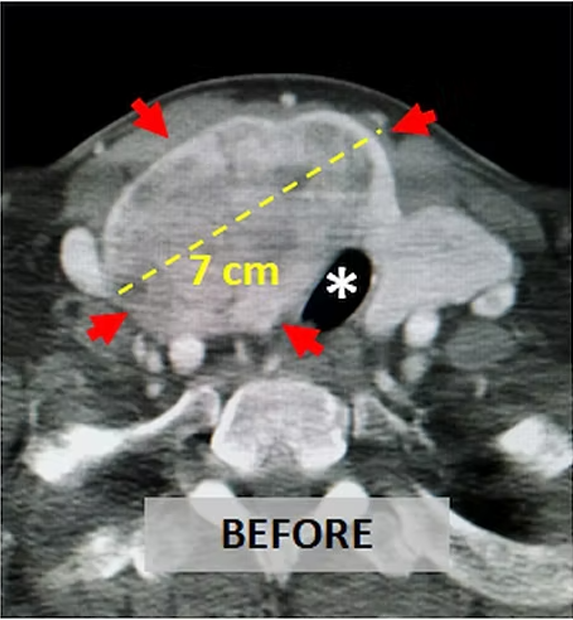
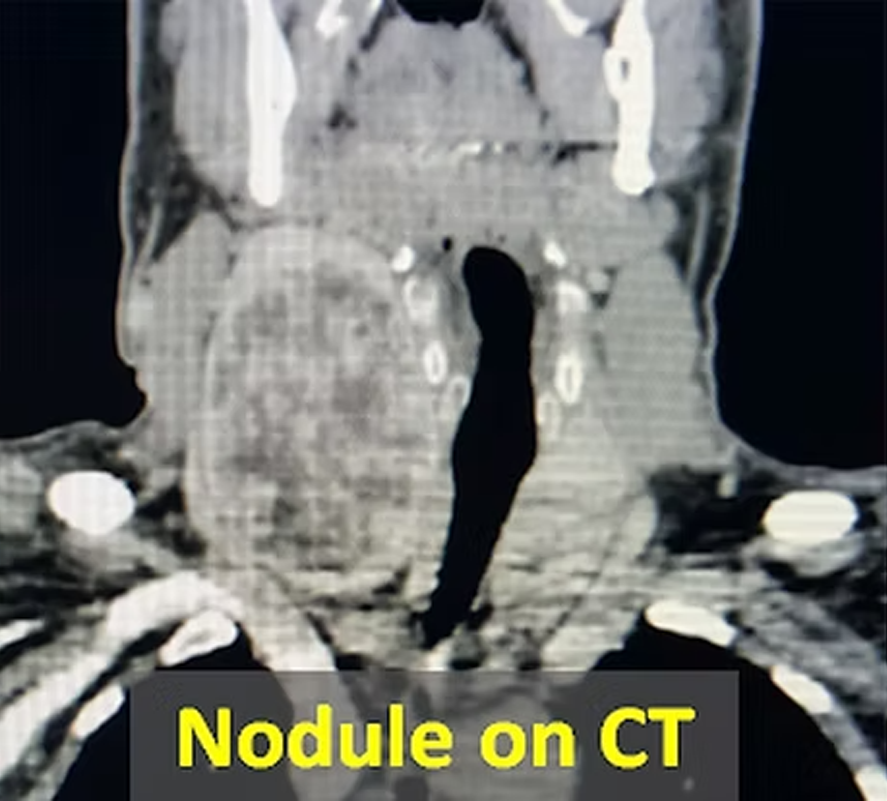
In our patient with a 7cm solid nodule in the right thyroid lobe that causes shortness of breath, snoring and sleep apnea; The nodule was treated with embolization by occluding its 2 feeding vessels in a simple angiography procedure.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
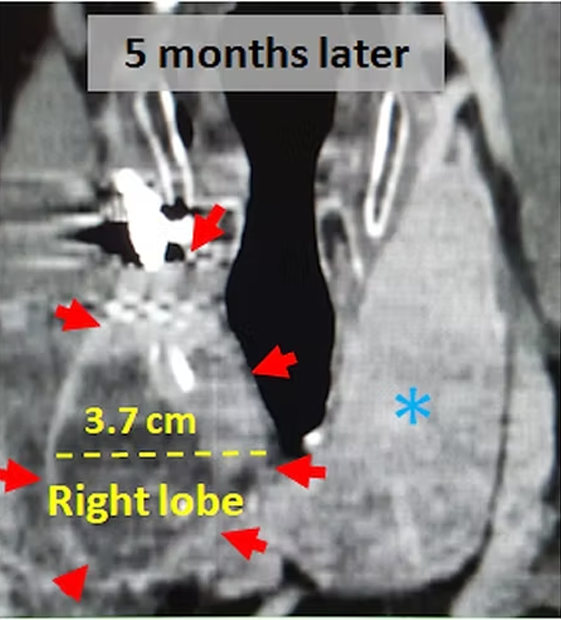
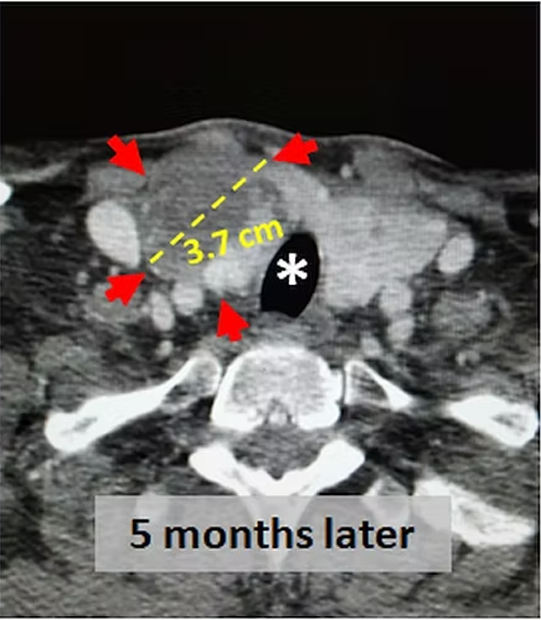
Five months after the treatment, the control CT images show that the diameter of the nodule was reduced from 7cm to 3.7cm, which corresponds to 86% volume reduction. The right lobe became smaller and as a result, its compression over the windpipe (*) became less. The normal left lobe (*) has enlarged as a compensation. After the treatment, the patient had no more complaints and his neck swelling disappeared completely.
How is embolization performed?
What are the advantages of embolisation?
İt is like a coronary angiography procedure. It is painless, done under local anesthesia and the patients stay in the hospital for one night only. It is very effective in large or plunging goiters, single large nodules and the Graves disease. Since the thyroid is not directly touched, there is 0% danger of voice loss due to recurrent laryngeal nerve damage.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
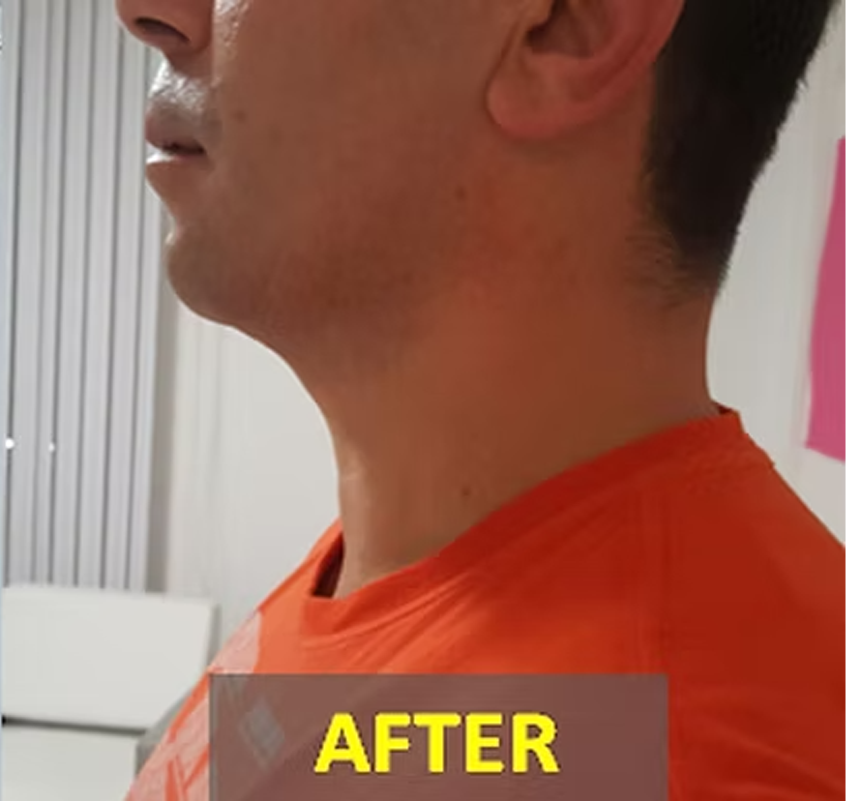
In our patient with a 9cm solid nodule in the right thyroid lobe, the nodule was treated with embolization. After the procedure, the nodule has shrunk and the cosmesis improved markedly.
Embolisation versus ablation?
If the thyroid has only a single nodule or severek nodules with a diameter of less than 6 cm in size, percutaneous ablation is generally the treatment of choice. If the nodules are too many or large (6cm), or there is a large/plunging goiter, then embolisation is much more practical and effective than percutaneous ablation.
Contact Us
You can get information on our treatments via phone and e-mail as well as by filling and sending the consultation form below. Please send the reports of your thyroid ultrasound, hormones, scintigraphy and biopsy (if available) via e mail (thyroidgoiter@gmail.com) or whats up ( +90-850-255 24 23). Remember to write clearly your e mail address and phone number so that we can return to you as soon as possible.
Please add the reports of your thyroid ultrasound, hormones, scintigraphy and biopsy (if available)