Thyroid Cancer
Thyroid cancer is seen quite frequently, and its incidence has been substantially increased in the last decade owing to the wide spread use of ultrasound and fine needle aspiration biopsy (FNAB). Thyroid cancer is 2.5 times more common in females and it is more frequently seen in patients who received radiotherapy to the neck and in those whose family member(s) have thyroid cancer.
There are 4 types of thyroid cancer.The most common types are papillary cancer (75-80%) and follicular cancer. These are very slow-growing tumors and survival is very long even in patients who have developed metastases. For this reason, papillary and follicular cancers are also called “well-differentiated” cancers. Since the survival is extremely long especially in papillary cancer, it is currently questioned whether or not aggressive treatments such as thyroidectomy is really necessary in this patient group. In general, 20 years survival is 98-99% in papillary cancer and 80-90% in follicular cancer.
How is diagnosis made?
Thyroid cancers generally do not cause any complaints. They are mostly diagnosed incidentally during a neck ultrasound examination that is done for goiter or for reasons other than the thyroid. Owing to the wide spread use of ultrasound, most thyroid cancers are diagnosed at an early stage. Although the vast majority of thyroid nodules are benign, some ultrasound features increase the likelyhood of malignancy (cancer). These include large (>1cm) size, irregular contours, hypoechoic (dark) appearance, increased vascularity, perpendicular orientation to the skin (taller than wide) and presence of microcalcifications.



Typical ultrasound features of papillary carcinoma: A. Taller than wide and hypoechoic appearance, large size. B. Irregular contours, large size, microcalcifications (white spots) and hypoechogenecity. C. Large size and increased central vascularity on color Doppler ultrasound. If these features are present on ultrasound, probability of cancer is considered high and a fine needle aspiration biopsy (FNAB) should be performed.
If the ultrasound appearance of the nodule(s) suggest malignancy a fine needle aspiration biopsy (FNAB) should be performed. This procedure is done under local anesthesia with ultrasound guidance and typically lasts for several minutes. FNAB is quite accurate and can successfully make the diagnosis in more than 70% of the cases. However, in about 15% of FNABs, the result is nondiagnostic, which means that the amount of cells aspirated is not enough to make a diagnosis. In another 15% (avarage) of FNABs, the result is indeterminate, which means the pathologist can not make the diagnosis confidently although the amount of aspirated cells is enough. In this 30% patient group, where FNAB is not successful, it is a common practice to repeat the biopsy. However, not uncommonly, the second FNAB is not able to provide the diagnosis. For this reason, some centers including ours, prefer to do a trucut biopsy additionally besides the FNAB in the second biopsy procedure. In this way, the pathologist can make the diagnosis much more accurately and confidently. What’s more, if the result is cancer, trucut biopsy allows to determine the subtype of cancer, which is important for both treatment and prognosis.
If the thyroid nodule(s) prove to be cancer with biopsy, the classic treatment is total thyroidectomy with or without radioactive iodine (RAI). In patients with small (<2cm) cancers confined to the thyroid, some centers have also used percutaneous ablation and reported excellent short and mid term results. At our center also, we prefer to treat papillary cancers with percutaneous ablation (cryoablation, RF or microwave) if the tumor did not spread out of the thyroid. We believe that this approach is more appropriate than the classic aggressive surgery given the very indolent course of the well-differentiated thyroid cancers.
{kind=link}
{kind=link}
{kind=link}
Papillary microcarcinomas (<1,5cm in size, no capsule invasion, no lymph node metastasis) can be safely and effectively treated with percutaneous radiofrequency, microwave or cryoablation.
Low risk papillary carcinoma
Nearly 3/4 of thyroid cancers are papillary carcinoma, and their majority are low risk tumors. Low risk papillary cancer (also called papillary microcarcinoma) is defined as a small (<1-1.5cm) tumor, that is confined to the thyroid and not metastasized to the neck lymph nodes. In such cases, survival rates are as high as 98% in 20 years. Today, with the increased use of ultrasound and FNAB, low risk papillary microcarcinomas are diagnosed more and more frequently, and it is believed that these tumors currently constitute about 80-85% of all papillary cancer diagnoses.
Despite their very good prognosis, papillary microcarcinomas are treated as aggressively as other thyroid cancers. In these patients, the standart of care is still total thyroidectomy plus RAI. However, many investigators believe that total thyroidectomy is too agressive and RAI does not have any benefit in such patients. Some authors even recommend no treatment for these tumors. In a study from Japan, 1465 low risk papillary carcinomas were followed up for 5 years without any treatment and only 5% of these tumors showed enlargement and only 2% developed lymph node metastases.
Another treatment that is recommended for low risk papillary carcinomas is percutaneous ablation. This method is preferrred increasingly by patients and some doctors because it does not have the risks of surgery and can kill the tumor completely, therefore, it provides a much more attractive alternative to the “no treatment strategy”.
{kind=link}
{kind=link}
{kind=link}
Laser or RF ablation of thyroid nodules
Advantages of percutaneous ablation in thyroid carcinoma:
1. It can completely kill the cancerous tissue in the thyroid.
2. The thyroid gland remains in place. Therefore, there is no need for life long hormone therapy.
3. The patient is not exposed to the risks of the surgical operation.
4. There wiil be no incision on the neck.
5. No hospitalization is required, it is an outpatient treatment.
6. If surgery is required for any reason in the future, it will not prevent the operation
Which ablation method is more suitable?
Radiofrequency ablation, microwave ablation and cryoablation techniques can be used in thyroid cancer. Radiofrequency and microwave kills cancerous tissue by heating it, and cryoablation by freezing at -140 degrees. Although we apply all three methods in our center, we prefer the cryoablation (freezing) technique in most of our patients. This is because cryoablation is painless, the ablation area can be seen clearly during the procedure, and larger tumors can be treated.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Why is cryoablation advantageous in thyroid cancer?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
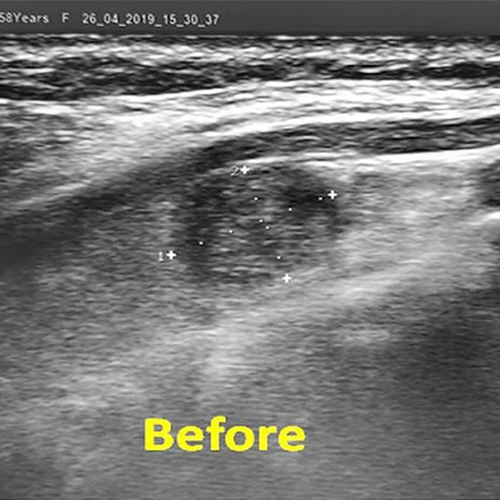
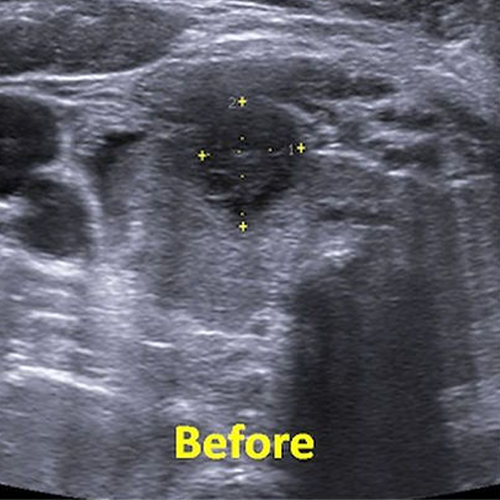
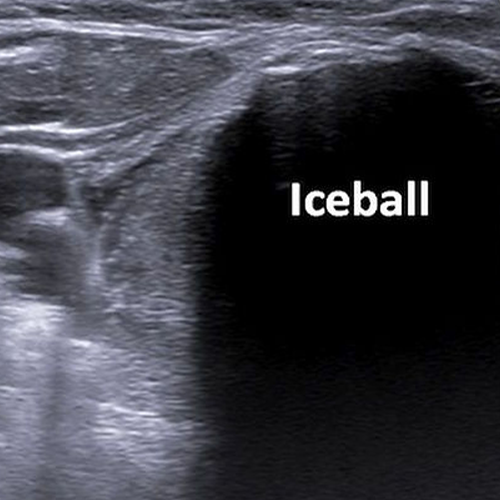
In a 40-year-old female patient with a 23 mm nodule in the right thyroid lobe, the FNAB result was slightly suspicious for carcinoma (AUS / FLUS). The patient underwent percutaneous cryoablation under ultrasound guidance. During the procedure, the nodule and a large area around it were frozen completely (ICEBALL). On ultrasound performed three months later, it was seen that the nodule became extremely small and turned into a scar tissue.
1. Since it is painless, we can do it with local anesthesia.
2. By having the patient talk, we can control his / her voice during the procedure.
3. We can clearly see where we freeze (ablation area) on ultrasound and tomography during the procedure. Thus, we can be sure that we cover the tumor completely and we can more easily protect the surrounding vessels and nerves.
4. Since the ablation area is larger, we can also treat cancers that are larger in size.
5. Since it does not damage muscle, cartilage and connective tissue, it is safer in tumors adjacent to these structures.
What to do if thyroid cancer is suspected in biopsy?
Pathology result yields cancer suspicion in a significant portion of thyroid fine needle biopsies (between 10-40%). This suspicion is graded according to a classification called Bethesda. In Bethesda 3 (AUS / FLUS), the probability of the nodule being cancer is 5-15%, in Bethesda 4 (follicular neoplasm or suspected follicular cancer) 15-30% and in Bethesda 5 (suspicious for cancer) it is between 60-75%. If one of these result come after the biopsy, the patient is recommended to either get the thyroid removed or follow-up and biopsy at short intervals.
However, both options start a troubling process for the patient. If the patient is operated on, he or she will lose the thyroid and will use hormone pills for life, and since the pathology result will probably be benign at the operation, the patients will have had an unnecessary thyroidectomy. In the follow-up + biopsy option, the patient will be biopsied at regular intervals for years. There are various scenarios in this situation: In most patients, some biopsies will reveal suspicious and some will reveal benign results and even if all subsequent biopsies after the first biopsy are benign, the suspicion of cancer will not disappear completely. Thus, the patient will have to live in anxiety for years. On the other hand, in a small proportion of such patients, it becomes clear years later that the patient has in fact cancer. In this case however, treatment may be delayed. For these reasons, we prefer to apply percutaneous ablation treatment in patients whose thyroid biopsy result is suspicious, if the size of the nodule is appropriate and there is no spread to the regional lymph nodes. We think that this approach will provide early treatment of the patient if cancer is present, save the patient from living in anxiety with suspicion of cancer, and prevent unnecessary removal of the thyroid.
If the cancer recurs in the neck after the operation, surgery may still be repeated. Alternatively, percutaneous ablation (laser, radiofrequency, microwave, alcohol) can be performed for the recurrent cancer foci. Many studies in the literature report good local control rates with ablation in recurrent thyroid cancers.
Many studies have shown that laser, radiofrequency and microwave are very successful in the treatment of low risk papillary carcinomas. Therefore, although the long term results are not very well-known, percutaneous ablation is an important treatment option in patients who is not fit for or do not desire surgery.
Thyroid cancer metastases
Thyroid cancers can metastasize to neck lymph nodes, lungs and bones. In these patients, classic treatments are surgery (if possible) and RAI. Recently, some studies have reported very good local control rates with percutaneous ablation in the treatment of recurrent lymph node metastases after surgery. Similarly, some authors also reported that distant metastases of thyroid cancers to the lungs, liver and bone can also be successfully treated with percutaneous ablation or embolization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contact Us
You can get information on our treatments via phone and e-mail as well as by filling and sending the consultation form below. Please send the reports of your thyroid ultrasound, hormones, scintigraphy and biopsy (if available) via e mail (thyroidgoiter@gmail.com) or whats up ( +90-850-255 24 23). Remember to write clearly your e mail address and phone number so that we can return to you as soon as possible.
Please add the reports of your thyroid ultrasound, hormones, scintigraphy and biopsy (if available)